I've been dealing with hernias since 2020. Looking back, it didn't start with a dramatic accident, but rather with a moment when the body suddenly sent a clear signal: Something is different. A hernia can announce itself in a surprisingly unspectacular way - until you can no longer ignore it. For me, it came relatively suddenly.
The first operation followed a few months later, but the journey was not „finished“. This is precisely why it is worthwhile to first understand the topic properly - as it is medically intended, and at the same time with a keen eye on the things that often fall by the wayside.



What is a hernia anyway?
A hernia (med: Inguinal hernia) is essentially not a „wound“, but a kind of weak point in the groin area. More precisely, it is a point in the abdominal wall where tissue gives way. Peritoneum can bulge through this gap - sometimes also with parts of fatty tissue or intestine. This sounds more dramatic than it often seems in everyday life: many people initially only notice a small protrusion, a pulling sensation, a feeling of pressure or a „strange“ feeling when straining.
What is importantA hernia is not simply „a hole“ that suddenly appears out of nowhere. It is rather the result of strain and a weak point - and this combination can build up gradually, even if the visible moment appears „sudden“.
Typical signs: From „just funny“ to clear
Many sufferers report similar patterns, even if the details vary:
- Protrusion in the groin, which becomes more pronounced when standing or pressing
- Pulling or burning, especially when lifting, carrying or coughing
- Feeling of pressure, as if „something is no longer quite stable“
- Sometimes also pain, sometimes surprisingly little pain - what can be deceptive
It is precisely this ambiguity that causes many people to hesitate at first: you don't want to overestimate it, you hope it will go away, you take it easy for a few days. That's human - but in the case of a hernia, „wait and see“ only makes sense if you really clarify what's going on at the same time.
Why does this arise from a medical point of view?
The classic medical model is basically understandable: There is pressure in the abdomen. This pressure increases with everything you do that „presses“ - lifting, carrying, standing up with difficulty, coughing, sneezing, constipation, intensive training, sometimes simply through permanently high basic tension.
If there is tissue weakness in the groin area, the pressure can „push through“ there. This weakness can be congenital, increase with age or be exacerbated by stress. The issue is particularly common in men because there are anatomical structures that make the abdominal wall „more complex“ at this point. (This is not a judgment, but pure construction).
The crucial thing about this view is that it is mechanical. And mechanical often makes sense in medicine in the first place - because it makes things tangible, measurable and surgically solvable.
Direct and indirect inguinal hernia: two variants, same construction site
Medically, a distinction is often made between:
- Indirect herniaThe fracture tends to run along a „natural path“ (via structures that are anatomically designed there).
- Direct herniaThe hernia is more likely to go through a weak point in the abdominal wall itself.
For everyday life, this distinction is less important than the consequence: in both cases, it is about stability in the transition area between the abdominal cavity and the groin. And in both cases, as soon as pressure is repeatedly applied unfavorably there, the body will eventually find its weakest point.
Why is surgery performed so often?
The honest answer: Because in many cases it is the most sensible solution. A hernia usually does not simply „grow back“ in a stable manner. It remains a weak point. And if parts of the intestine become trapped, it can become an emergency. The medical logic is therefore clear: if a hernia has been diagnosed and is causing symptoms - or a risk is recognizable - then surgery is often the pragmatic way forward. This is also a classic, tried and tested way of thinking:
- If something is structurally unstable, you stabilize the structure.
- Either by stitching, by reinforcement or by a net.
And yet a skeptical but fair thought is worthwhile here: the operation repairs the spot - but it does not automatically answer the question of why the print landed there so awkwardly in the first place.
Why the mechanical model often falls short
This is where the part that is often missing in the mainstream begins - and which will become important later in my article. Because even if you acknowledge that surgery often makes sense, questions remain unanswered:
- Why do some people get a hernia even though they have done „nothing special“?
- Why does a hernia come back after a short time in some cases?
- Why do some people feel stable quickly after surgery, while others take a long time?
- Why is the bar sometimes just „the end of a chain“?
To be honest, medicine often works with a shortcut here:
„Weak point + pressure = break.“
That's true - but it's only half the story. The other half is the question:
Why is the pressure the way it is?
And more importantly, why is it distributed in this way? The body is not a machine with a single defective part. It is a tension and static system. Pressure is not only caused by „weight“, but also by posture, breathing, muscle tone, stress patterns and movement habits. You can ignore this and still operate successfully. But if you want to understand why some processes are complicated, it is almost impossible to ignore these factors.
The groin as a transition point: anatomy meets everyday life
The groin is not an isolated place. It lies at a kind of crossroads:
- Above the abdominal cavity with its pressure system
- Pelvis and hips bearing the load at the bottom
- Lateral muscles and fascia that distribute tension
- inside the structures, which are different for men and women
It is precisely such transitions in the body that are often more sensitive than „smooth surfaces“. This is also familiar from craftsmanship: where forces are redirected, where there are material transitions, where constructions become complex - this is where weaknesses first become apparent.
Anyone who accepts this comparison will immediately understand: it is logical that it can „happen“ in the bar. But it is just as logical to ask why it happens to some and not to others.
This first chapter is not intended to impose a theory, but to lay the foundations:
- An inguinal hernia can be well explained medically and can often be operated on sensibly.
- The mechanical model is correct - but often incomplete.
- The bar is a transition point in a larger system of pressure, tension and statics.
Anyone who experiences relapses, long periods of rehab or strange feelings of pressure often has reason to look not only at the groin, but also at the „surrounding area“. In the next chapter, I will therefore delve into my own story: two operations, two methods, two very different experiences - and the question of what all this has to do with stability, which not only needs to be „sewn up“ but also lived.

Inguinal hernia: Recognizing warning signs & symptoms - Causes & treatment of an inguinal hernia | DoctorWeigl
Two operations, two paths - and why trust plays a role here
After the first chapter, a lot of things sound logical at first: weak point, pressure, surgical stabilization. That's how you think, that's how it's explained, that's how it's done - and in many cases it works. However, as soon as you are affected yourself, there is a second level that is often missing in guidebooks. It's not just a medical problem, but also a confidence problem. Because if an operation doesn't have the desired effect, it changes something. People become more cautious. More skeptical. And at the same time forced to take a closer look.
My own story with the hernia is therefore not just a „surgery story“. It is also a story about how you reassess what you can still trust your own body - and the system - to do after a setback.
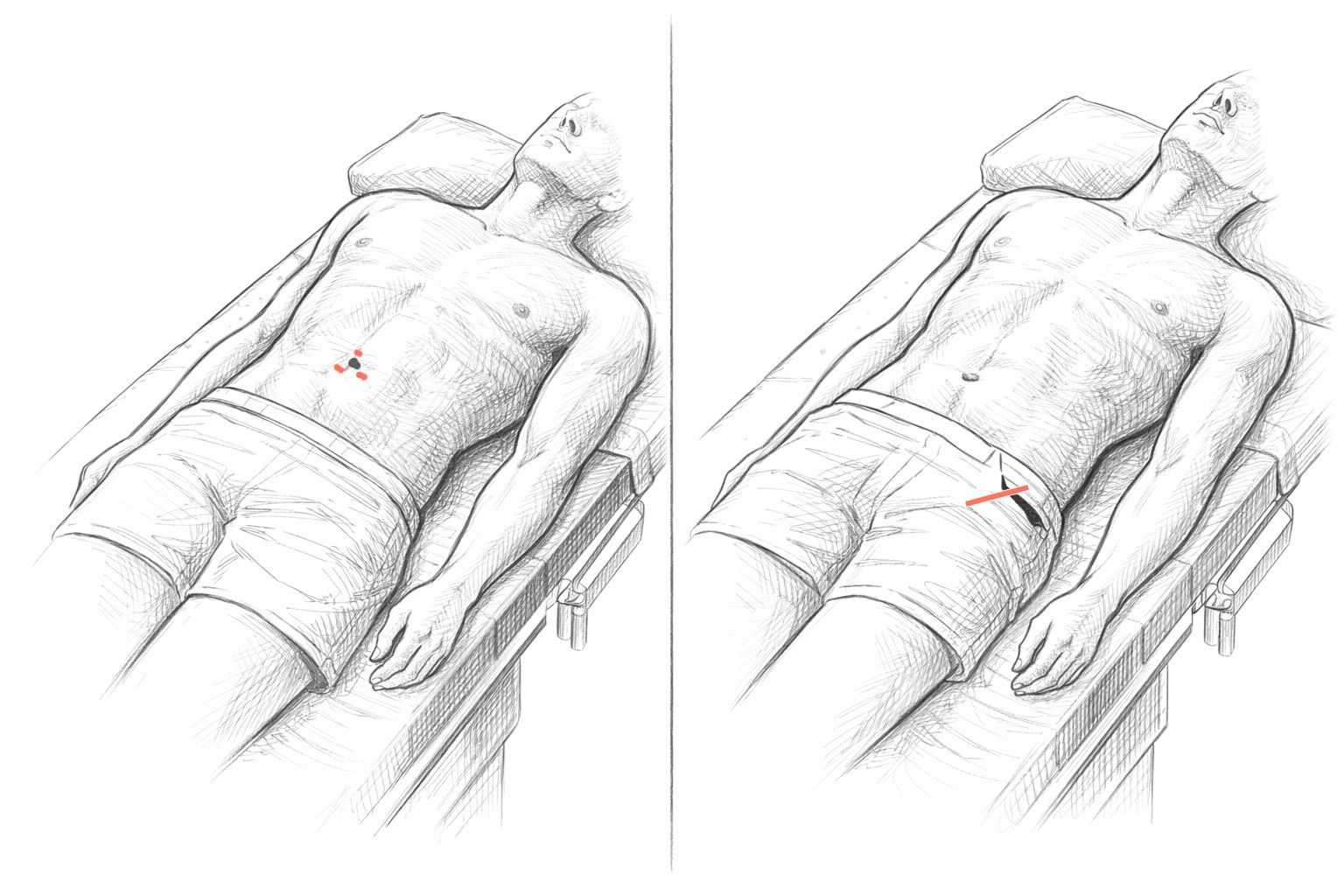
2020: The first operation - bilateral, laparoscopic „through the abdomen“
The first operation was in 2020, on both sides. Laparoscopically. In other words, what is often considered the modern standard today: minimally invasive, small incisions, camera technology, access via the abdominal cavity. If you only read the theory, it sounds very convincing. Less wound area, faster recovery, technically elegant, often described as „gentler“.
And yes, many people get on well with it. I want to say that explicitly because I don't want to convey the message that this method is fundamentally bad. But for me personally, this operation was much more unpleasant than I had expected. Not in the sense of „drama“, but in the sense of: It simply didn't feel the way I had imagined „gentle“ to be.
This is a point that is worth making: „minimally invasive“ does not automatically mean „minimally invasive“. It just means fewer incisions from the outside. The body still notices what happens on the inside.
Why „modern“ does not automatically mean „better“
In medicine - as in technology - there is a natural tendency: newer procedures are often perceived as progress, partly because they can objectively have many advantages. But progress is never simply „better“. It is often: different. And „different“ can be better or worse for the individual patient.
During laparoscopic groin surgery, access is gained via the abdominal cavity. This affects areas that are otherwise not even on the patient's radar. You can feel it in the way your body reacts afterwards: Abdomen, feeling of pressure, movements, sometimes also a very general feeling of „something has happened inside“. It's difficult to describe, but many patients immediately understand what is meant.
And this is where the first important learning experience begins: not every method feels the same as the brochure suggests.
The relapse: the hernia was back after three months
And then came the point that changed everything: After about three months, the hernia was back. That's not just a medical fact - it's a psychological turning point. Because as a patient, you initially think: „Okay, that's been fixed now. Now I can check it off.“ When it comes back so quickly, the first reflex is often: What's wrong here?
Important here isA relapse can have many causes. This does not necessarily mean that „bad surgery“ was performed. It may be that the tissue has reacted unfavorably. It may be that the strain came too early without you feeling it was „too early“. It may be that the original weak point was larger or more complicated than expected. Or there are factors that hardly appear in the standard model: Posture, pressure distribution, chronic tension, pelvic position, breathing.
But no matter what the cause was, one thing happened at that moment - trust was lost. And that is human. You become cautious. You listen to yourself. You start to evaluate every cough, every movement, every carry. And suddenly everyday life can no longer be taken for granted.
Three years of „running around with it“: Not out of stubbornness, but out of insecurity
After this experience, I walked around with a damaged groin for three years. Not because I wanted to be heroic, and not because I'm „against surgery“. But because I was insecure. Once something hasn't worked, you automatically ask yourself questions that didn't matter before:
- What if it happens again?
- What if the cause is not there at all?
- What if I just keep repairing in the same place without understanding the basic problem?
- What if my body is trying to tell me something about my stress, posture or tension - and I'm not listening?
These are not esoteric thoughts. It's simply common sense: if a solution doesn't hold, you start to look at the problem differently. And this is an important point that many people underestimate: It is often not the pain that is the biggest problem, but the constant insecurity. You limit yourself, you avoid movement, you develop a kind of inner protection program. This can be useful - but it also costs quality of life.
2023: The second operation - left, classic, „the old way“
In the summer of 2023, I decided to have a second operation. This time only on the left - and this time using the conventional method (open method according to Lichtenstein), i.e. with a direct cut. Exactly the method where many people say: „It's more difficult, it's bigger, it's more stressful.“ That's exactly what I was told: that the classic method is more time-consuming.
And now comes something that was surprising for me: I found this second operation much less unpleasant than the first laparoscopic one. Of course, this is subjective - but that's exactly why it's so valuable to talk about it. Because it shows: Medical assessment („more difficult“) and patient experience („more unpleasant“) do not have to be congruent.
This operation was actually successful. It holds. And that is a crucial point: not because I am now „against modern“, but because it shows that the classic, tried and tested method has its good reason. There are procedures that have been used for decades because they work - not because there are no better ideas, but because they are robust in real life.
The „fat“ break: when the problem is no longer small
Another aspect: I had a really big hernia on the left. This is not just a side note, but an important background. Because a small, incipient hernia feels different to a full-blown hernia. And the decision to have surgery also feels different.
When you realize that it's no longer „a bit of pulling“ but a clear instability, the benefits of surgery become more important. At the same time, however, there is also more concern: „If it comes back now, what then?“
Such thoughts are normal. And they belong in an honest article - because many readers know them quietly, but hardly anyone expresses them openly.
After the second operation: success - but not immediately „everything as before“
Even after the second, successful operation, everything was not suddenly resolved. I still had regular problems in the first few years. Carrying was difficult. Weight-bearing was tricky. And it didn't just last a few weeks or months, but rather one to two years - maybe even longer if you look at it honestly.
This is a point that is missing in many short texts: you often read „back to full strength after X weeks“, and then those affected are surprised when the body doesn't stick to it. But the body is not a checklist. Structure and function do not always develop at the same pace.
It may be that the surgery is stable, but the rest of the body - muscles, fascia, movement patterns - is still in a protective mode. You move differently, you hold differently, you unconsciously tense differently. And as long as these patterns continue, there is a residual risk that pressure will again have an unfavorable effect or that symptoms will persist even though „everything has actually been repaired“.
If I had to summarize this chapter in one key point, it would be this:
- Surgery may be useful and necessary.
- A relapse can happen - without having to immediately look for someone to blame.
- However, a relapse changes the perspective: you ask deeper questions about the causes.
- Classic methods are not outdated, but often simply tried and tested.
- Success does not automatically mean that the body immediately functions „normally“ again.
And above all: after two operations, one question remains that has stayed with me for a long time and will play a central role later in this article:
If the groin was the weak point - why did the pressure get there in the first place?
This is exactly where the next chapter comes in. Because after the successful second operation, the really interesting phase begins: life afterwards - and the realization that stability is not only „stitched“, but also has to do with statics, posture and pressure distribution.
The following illustration shows a comparison between laparoscopic surgery „through the abdomen“ (left) and classic open surgery (Lichtenstein method):
When the surgery holds, but the body still needs time
After the second operation, I was initially relieved. The large left inguinal hernia had been repaired, the wound had healed and, medically speaking, everything was fine. And yet a feeling arose relatively quickly that many patients know, but rarely talk about: The structure was stable, but confidence in their own body had not yet returned.
You get on with your life, you function, you get things done - but in the background there is a constant internal comparison going on: Can I lift this? Should I turn like this? Was that already too much? This phase is not spectacular, but it has a greater impact on everyday life than any acute episode of pain.
The time after the operation: caution instead of ease
In the months following the second operation, I realized that „successfully operated on“ is not the same as „able to bear weight again as before“. Carrying remained difficult. Not in the sense of immediate pain, but rather as a subliminal warning from the body. It was this vague feeling that you had better be careful - even if there was nothing objectively wrong with it.
Looking back, this was not a weakness, but a form of self-protection. The body had learned that the groin is a sensitive area. And this learning does not simply disappear just because a surgical procedure has taken place. Muscles, fascia and movement patterns need time to reorganize themselves.
Why aftercare is often only half the battle
Medical aftercare is generally focused on clear parameters: Wound healing, stability, no complications. This is sensible and necessary. What is often missing, however, is a look at the functional interaction. How does someone move after the operation? How is tension distributed when standing up, coughing, carrying? Which postures have crept in?
These questions are rarely asked because they are difficult to measure. They cannot be dealt with in a short check-up appointment. And yet they decide whether someone will move again as a matter of course after months - or remain cautious in the long term.
For me, this phase lasted longer than I would have expected. Not weeks, but rather years. Two, maybe even three years, during which I consciously avoided a lot of things. Heavy shopping, awkward movements, anything that was „jerky“. This had nothing to do with panic, but with experience. Once you've experienced how quickly a hernia can come back, you don't get careless.
At the same time, this is not a state that can be maintained forever. Because permanent caution changes the body. You compensate. You tense differently. You shift stress to other areas. And this is where a silent cycle begins that many people don't notice: The original weak point is repaired, but the overall system remains imbalanced.
Structure is repaired - function must be found anew
An important thought that only became clear to me over time: An operation repairs structure, not automatically function. Structure means: the tissue holds, the mesh fits, the suture is stable. Function means: how forces move through the body in everyday life.
If function and structure do not come together again, a kind of inner tension arises. The body behaves as if the danger is still there, even though it has been objectively eliminated. This is not a psychological problem in the narrower sense, but a deeply rooted protective mechanism. The body „remembers“ stress - and reacts with appropriate caution.
The role of habits and unconscious tension
During this time, I realized how much everyday attitudes and habits are underestimated. How you stand. How you sit. How to stand up. How to distribute loads. Much of it is automatic. But after an operation, this automatism is often disturbed. You unconsciously hold your stomach tighter. You avoid certain movements. You tense up where you should actually let go.
The problem with this is that permanent tension creates pressure again. Not always where you feel it, but often at transitions. And it is precisely these transitions - such as the groin - that react sensitively to unfavorable pressure conditions.
Why time alone does not solve everything
There is this widespread thought: „It'll get better with time.“ And yes, time is important. But time alone is not always enough. If unfavourable patterns become entrenched, time can even stabilize them. The body then learns not „relaxation“, but „permanent tension as a normal state“.
For a long time I had the feeling that something fundamental was not yet right - without being able to put my finger on it. The groin held. But it didn't feel natural. And it's precisely this feeling that you should take seriously instead of pushing it away.
This chapter marks a turning point in understanding. It is no longer about the question of whether surgery should be performed or how it was performed. It is about the aftermath. It's about the space between medical success and physical suitability for everyday life. My most important realization from this phase was:
- Stability comes not only from repair, but also from functioning interaction.
- Caution makes sense, but can create new problems in the long term.
- The body not only needs time, but also the opportunity to realign itself.
This is exactly where the next step begins: the question of what actually changes in the body when you intervene in a seemingly completely different place. In my case, this was the CMD splint - and with it a change in statics that went far beyond the jaw.

CMD splint, statics and the body as a whole
If you wear a CMD splint for four years, you learn something that you would hardly believe before: The body is not a construction kit in which you replace one part and the rest stays the same. Of course, everything starts in the mouth - with the bite position, jaw joint and muscles. But the longer this kind of therapy goes on, the clearer it becomes: The jaw is not just a jaw. It is part of a system that runs through the entire body.
And this is exactly where it got exciting for me. Because while I originally „only“ wore a splint because of CMD, I noticed more and more clearly over the years that something fundamental had shifted in my statics. Not quickly, not spectacularly - more like a house settles minimally when a load-bearing element changes. Only gradually do you realize that the weights are different.
What a CMD splint actually does - in simple terms
A CMD splint is often described as follows: it relieves the jaw, guides the lower jaw into a more favorable position, soothes the muscles and protects the teeth. That is all true. But this description makes it seem as if the splint is a local aid - like a plaster on the skin.
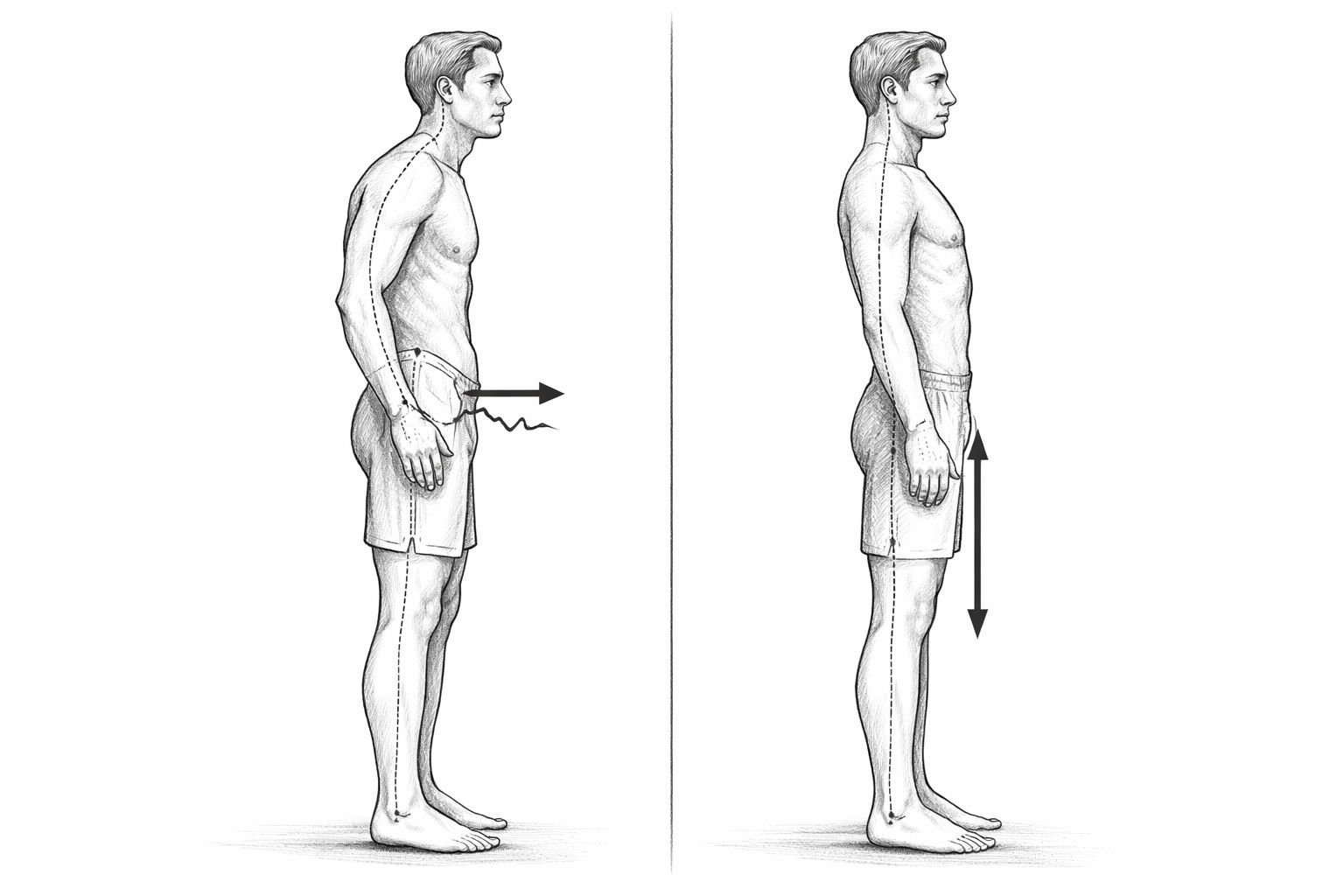
In reality, it interferes with something much deeper: the bite position. And the bite position is not a detail. It is a reference point to which the body orients itself. Because the head is not simply „on top“. The head is a heavy, movable weight - and the body must constantly keep it in balance. When the position of the jaw changes, it often changes too:
- how the head sits on the cervical spine
- how the neck muscles work
- How to maintain tension in the shoulders and chest
- how the body is „erected“ overall
None of this happens with a bang. It happens slowly. And that is precisely why it is often underestimated.
The body functions in chains, not in individual parts
An important thought that I only understood over time: The body works in chains of tension. This means that if something changes at the top, areas at the bottom also react. And if something is wrong at the bottom, the top compensates.
This is not an exotic idea. It's actually the oldest approach of all: if you had a crooked door in the past, you didn't tinker with the handle, you looked to see if the frame was warped. The human body works in a similar way. If a system is out of kilter, it tries to balance itself out everywhere.
And this is precisely why it is plausible that a splint - if it changes the bite position in the long term - not only „protects teeth“, but can also promote new statics over the years.
Why changes often only become visible years later
Many people expect a clear effect from therapies: before/after. But static in particular is often a long-term process. It was the same for me. I didn't say after three weeks: „Now my pelvis is in a different position.“ It doesn't work like that. It's more like a ship that you set on a new course: the deviation only becomes visible after many kilometers.
With a CMD splint, the body not only has to accept a new position, it also has to stabilize it. That is work. Muscles, fascia and movement patterns have to reorganize themselves. And this reorganization can also result in new sensations over a longer period of time: In some places it gets better, in others you temporarily feel more.
That's one of the reasons why I remain skeptical about such topics: it's very easy to draw „conclusions“ too early. But over four years, it becomes more difficult to dismiss everything as just a coincidence.
In a separate article, I have summarized how the final phase of CMD treatment with a functional splint.
Head, jaw, spine: the top pulls the bottom down
The jaw is functionally connected to the cervical spine. Anyone who has ever had neck tension and jaw pressure has felt this. If the head is not well balanced, the muscles have to compensate permanently. Permanent compensation creates tension. Tension continues downwards. This can continue downwards:
- Shoulder girdle
- Chest
- Diaphragm region
- Lumbar spine
- Basin
These are not magical lines in the body, but real functional relationships. And if there is actually relief at the top, something can „follow suit“ at the bottom. The pelvis is particularly interesting here because - like the groin - it is a transition point. This is where forces from above and below meet.
Current survey on CMD symptoms
The pool as the pivotal point
The pelvis is particularly important in connection with groin problems. This is because the groin is located exactly where the abdominal cavity is connected to the pelvic and hip system. If the position of the pelvis changes, it also changes:
- the tension in the lower abdomen
- the direction of pressure when coughing, pressing or carrying
- the way in which loads „pass through“
- the sensation of stability in the groin region
And this is where my own observations come into play: Over the years of splint therapy, I increasingly had the impression that my pelvic position was changing. Not as a theory, but as a feeling in everyday life: how I stand, how I walk, how I shift weight.
I want to formulate this deliberately carefully: This is not a scientific statement in the sense of „rail shifts the pelvis by X degrees“. But it is a long-standing, repeated perception that fits in with other observations - and which cannot simply be wiped away.
Why this hardly plays a role in conventional medicine
This is where it gets interesting - and also a little uncomfortable. Because in traditional medicine, people often think in terms of responsibilities: the dentist does the jaw. The orthopaedist does the back. The surgeon does the groin. Everyone does their part - and that's understandable, because otherwise medicine would be almost impossible to organize.
But precisely this system has a weakness: it often does not see what happens between the areas. The „in-between“ becomes a blind spot. And chronic issues such as CMD, static problems or recurring pressure complaints often live precisely in this in-between space.
This does not mean that medicine is „bad“. It just means that it is strong in acute care and structural repair - and often less strong when it comes to long-term functional relationships.
An important clarification: This is not a promise of a cure
It is important for me to make something very clear at this point: A CMD splint is not a „hernia therapy“. I am not saying that it is: „Wear a splint, then it will go away.“ The body is not that simple.
What I can say, however, is that if the statics of the body change over the years - regardless of what causes this - then the pressure distribution can also change. And if pressure distribution changes, then this can explain why certain complaints shift or decrease. This logic is sober, classical and comprehensible:
- Forces do not act randomly in the body.
- Pressure looks for ways.
- Weak points are where pressure is applied unfavorably.
- When the paths change, the weak points change.
This chapter is something of a bridge between the „groin“ and the „overall system“. Because from here on, it becomes clear why I think differently about my groin problems today than I did in 2020. Not because I suddenly needed new convictions, but because an observation became apparent over time:
It's not just the bite that changes with the splint. Over time, the whole body changes - and therefore also where pressure is applied and how stability is perceived. The next chapter takes a very concrete look at a small but surprisingly significant detail: the cough. This is because it sometimes shows more clearly than any theory where the body actually directs the pressure - and how this pressure point can shift over the years.
When the pressure shifts - why statics often explain more than symptoms
Sometimes it's not measurements, images or diagnoses that help you, but simple everyday observations. For me, one of these was coughing. Something so banal that you don't normally pay any attention to it. And yet, over time, it was precisely this moment that made something visible that no examination could have shown me so clearly: The pressure point in my body had changed.
Such changes are not evidence in the scientific sense. But they are indications. And indications should be taken seriously - especially if complaints persist for years or keep recurring.
Coughing as a „pressure test“ of the body
Coughing creates high pressure in the abdomen for a short time. This is a completely natural mechanism. The body has to absorb and distribute this pressure. And this is exactly where the tension is and where the weak points are.
A few years ago - long after my second groin operation - I felt this pressure very clearly in my groin when I coughed. Not pain in the strict sense, but a clear focus: the body directed the pressure exactly there. This matched my experience at the time: although the groin had been operated on, it was still a functionally sensitive area.
Today it's different. When I cough, I feel the pressure more in the middle abdominal area, roughly below the navel. The groin is less and less noticeable. And it is precisely this shift that is interesting - not spectacular, but significant.
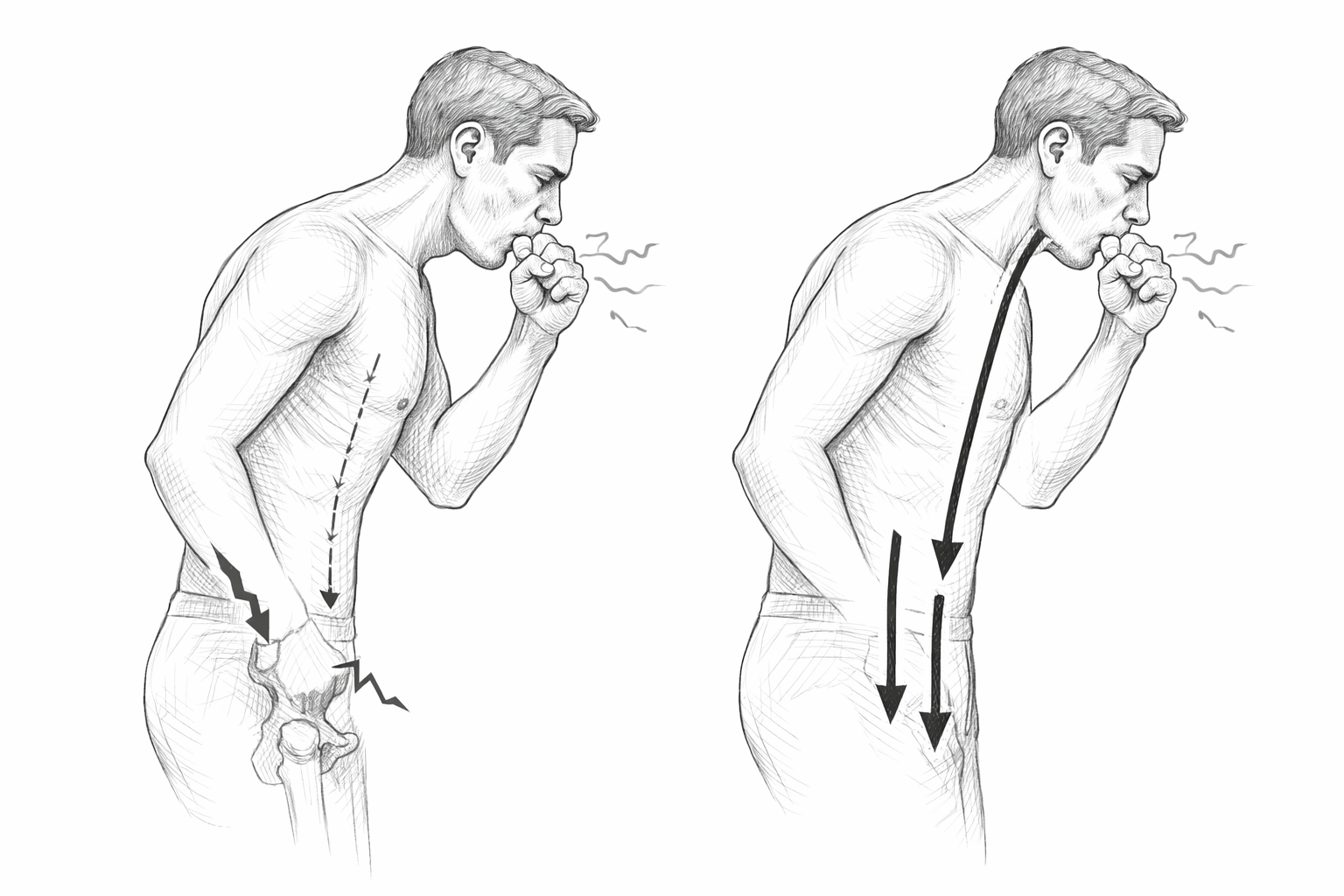
Pressure does not disappear - it seeks ways out
This is a central idea that you have to keep reminding yourself of: Pressure in the body does not simply disappear. It is redirected. When an area becomes more stable or is better integrated, the pressure looks for another path. This is not a mistake, but a sign that the system is working. If you understand this, many complaints become easier to understand:
- Why problems „migrate“
- Why symptoms disappear, but new ones appear elsewhere
- Why some therapies seem to help, but not permanently
The body is not a static object. It is a dynamic structure of tension. And that is precisely why it is so important not just to treat individual areas, but to look at the interplay.
Groin, pelvis, abdomen: a sensitive triangle
The groin region is located in a particularly sensitive area. It connects the abdomen with the pelvis and legs. This is where pressure from above, pressure from below and tension from the side meet. If something gets out of balance in this triangle, it often shows right here.
This does not only apply to hernias. Also Hemorrhoids, recurring lower abdominal pain or a constant feeling of pressure in the pelvic area can be an expression of the same problem: The pressure is unfavorably distributed.
And this is the point at which you should stop just looking at the symptom. Because if something keeps recurring, it's worth asking why the body sends the pressure there of all places.
Why statics is not an exotic concept
For many people, the term „statics“ sounds like a building site or architecture, not medicine. Yet it is actually very down-to-earth. Statics describes nothing other than the relationship between forces in a system. And the human body is such a system - only much more complex than a building. If the statics are right:
- load is distributed more evenly
- individual areas have to compensate less
- movements feel more natural
If the statics are not right:
- local overloads occur
- transition points come under pressure
- symptoms often show up where you least expect them
This is not an alternative idea, but a classic one. In the past, such correlations were often understood more intuitively because people paid more attention to posture, movement and stress in everyday life.
Recurring complaints are an indication, not a failure
An important point that puts pressure on many of those affected: when a problem returns, it quickly feels like a personal failure. „I must have done something wrong.“ „I didn't take it easy enough.“ „I wasn't paying attention.“
This falls short of the mark. In many cases, recurring complaints are not a sign of indiscipline, but an indication that the cause has not yet been fully understood. The body doesn't report symptoms to annoy you, but to indicate something.
Especially with issues such as hernias or hemorrhoids, which have a lot to do with pressure, it is worth taking this message seriously - without falling into fear or actionism.
Why it can be useful to get support
This is where a very practical recommendation comes into play. If complaints keep recurring or only partially improve, it can be very helpful to see someone who looks at the body as a whole. This could be, for example:
- an experienced osteopath
- a therapist with in-depth knowledge of body statics
- an orthopaedic surgeon who not only reads images, but also observes movement
The title is less important than the approach. The decisive factor is whether someone is prepared to ask questions such as:
- What is your position?
- How do you move?
- How do you breathe under stress?
- Where do you feel tension, even if it doesn't hurt?
Such conversations can be unfamiliar, especially if you come from a very technical medical background. But they often open up new perspectives - not as a substitute, but as a complement.
No quick solutions, but new clarity
Again, this is not a promise of a quick cure. Statics cannot be „repaired“ like a component. It changes over time - through awareness, through small adjustments, through new movement patterns. That takes patience. But it brings something that many people miss: Understanding.
If you understand why your body reacts, you often lose a large part of your anxiety. And those who have less anxiety tense up less. That alone can make a difference.
This chapter brings together the previous ideas and adds a practical consequence:
- Inguinal hernias and hemorrhoids are often the result of pressure problems.
- Pressure problems often have to do with statics.
- Statics cannot be considered in isolation.
- Those who only treat symptoms may overlook the underlying pattern.
To concern oneself with one's own body statics does not mean turning away from medicine. It means complementing it - with a view that used to be taken for granted and is often lost today.
The last chapter is therefore about categorizing these findings: without promising a cure, without apportioning blame, but with the question of what we can fundamentally learn from hernias - for our own bodies and for dealing with health in general.

Groin pain or even a hernia? That's what matters | Your fasciae
What you can learn from hernias
There are health problems that not only change your body, but also your outlook on life. A hernia is one of them for many people - not because it is always dramatic, but because it can be so stubborn. Especially when it comes back, when operations are technically successful but you don't feel safe in everyday life for a long time, a thought quickly arises that you hardly tell anyone:
„I may never get rid of this.“
I also had this thought at times. Not as panic, more as sober concern. Because I experienced how quickly a relapse can happen and because I felt for years that the groin remained a sensitive spot. It is therefore all the more remarkable that the picture has now changed - not suddenly, not through a „miracle cure“, but through a development that I would not have expected beforehand.
The most important insight: symptoms are often only the visible tip
When I look back today, I see that the hernia was a localized event - but the groin problems were probably part of a larger pattern. The groin was the place where it became visible. But the cause need not have been there.
This is an unfamiliar thought at first, because we like to make clear distinctions in everyday life: Here is the problem, there is the solution. But the body doesn't work like that. It compensates. It distributes burdens. It evades. And when a system is out of balance for a long time, the weakness often shows up where the pressure is most unfavorable.
This does not mean that every inguinal hernia is automatically „static“. It just means that if something recurs or lingers for a long time, it is worth looking further than the local site.
Surgery is not a mistake - it is often the necessary step
It is important for me to make this clear: I do not see operations as a „failure“ or as something that should be avoided at all costs. On the contrary: in many cases they are useful, sometimes unavoidable, and they save quality of life. Simply ignoring an unstable groin is rarely wise.
My second operation was also successful. It is holding. That's a good, solid basis. And that's exactly how you should look at it: Surgery can make the structure stable again. It creates the conditions in the first place for the body to be functionally restored. The problem often only arises when you think it will: „The operation was it, now everything is done.“
Sometimes this is true. But sometimes the body also needs a second step: a functional reorganization.
The unexpected part: that things sometimes work out after all
What surprised me the most was that the groin problems only improved noticeably in a period of time when I no longer expected it. I had long since adjusted to the fact that the groin would „remain a construction site“, which is constantly on my mind in everyday life.
And then the CMD splint treatment - especially in the second half of the treatment - set something in motion that I hadn't planned: I noticed how the statics were continuing to change, how the body was adjusting, how the pelvic position, balance and feeling of pressure were being rearranged.
I am not a doctor. I have no laboratory data, no series of measurements. I just have something that is sometimes more valuable in everyday life than any theory: long-term observation of my own body. And this observation is: the more the overall statics stabilize, the less the groin reports.
Why this hope is important - especially for chronic issues
Many people are looking for a kind of „end point“ for long-term complaints: a clear diagnosis, a clear measure, a clear cure. That is understandable. But with static and tension issues in particular, the path is often different. It is gradual. And sometimes improvements don't happen where you expect them.
This may be uncomfortable - but it is also good news. Because it means that if something doesn't improve for a long time, it doesn't automatically mean that there is no solution. It can also mean that you've just been looking in the wrong place.
And that is precisely the point at which the view opens up again: Away from the question „What's broken?“ to the question „What is connected to what?“.
A practical idea: check statics instead of just managing symptoms
If you want to derive something from my story, then it is a very down-to-earth thought:
Anyone who has recurring problems in the lower abdominal/groin/pelvic area - whether hernia, haemorrhoids or other pressure issues - can benefit from having their own statics looked at seriously. Not as a substitute for surgery or diagnostics, but as a supplement. This can mean
- Have movement patterns observed
- Understanding pelvic position, trunk tension and breathing
- find out where the body is permanently compensating
- talk to an experienced osteopath or an orthopaedist with an affinity for statics
Not every therapist is suitable for this, and not every method is automatically helpful. But the perspective alone can change a lot: If you understand that the body redirects forces, you no longer see complaints as a coincidence, but as a signal.
What I would do differently today - without being a know-it-all
When I look back on 2020 with the knowledge I have today, I would take a calmer approach to some things. Not in the sense of „I should have avoided the operation“, but in the sense of: I would have accepted earlier that the groin was perhaps not the cause, but the „alarm bell“. I would have asked myself the question earlier:
- Where does the basic tension come from?
- How is my tank positioned?
- How does my pressure line run under load?
- How do I breathe when carrying, when coughing, when stressed?
And I would have allowed myself earlier to look not only for the fastest medical solution, but also for the most sustainable one.
This is not a criticism of doctors. It's just an attempt to take your own body seriously - even where the system naturally can't cover everything.
Conclusion: Health is often a path, not a switch
If I were to end this chapter - and therefore the whole article - on a positive note, it would be this:
Yes, hernias can be stubborn. Yes, they can be unsettling. And yes, at times you can think you'll never get rid of it. But my experience shows that there are often solutions - sometimes even where you weren't looking for them.
For me, it wasn't the one perfect moment, not the one „miracle measure“, but a development over time: surgery as a structural basis, then patience, then - unexpectedly - a noticeable improvement due to the change in overall statics as part of the CMD treatment. That is the real message for me today:
You don't have to understand everything immediately in order to make progress. But you should be prepared to think beyond the obvious. The body is a system. And if you look at it as a system again, new paths often open up - sometimes quietly, sometimes slowly, but noticeably in the end.
And therein lies a comforting, almost old-fashioned thought:
The body has an amazing ability to reorganize itself - if you give it time, understanding and the right impulses.

Frequently asked questions about hernias
- What exactly is a hernia?
An inguinal hernia is not an open wound, but a weak point in the abdominal wall in the groin area. This weak point can cause the peritoneum, fatty tissue or, in unfavorable cases, intestines to bulge outwards. The cause is usually a combination of pressure in the abdominal cavity and a structural or functional weakness at this point. - Does a hernia really develop „suddenly“?
It often feels as if it comes on suddenly. In many cases, however, the weakness builds up over time. The moment you notice it is often just the point at which the body can no longer compensate for the strain and sends a visible or tangible signal. - Is surgery always necessary for an inguinal hernia?
In most cases yes, at least in the long term. An existing hernia does not usually close by itself. Surgery serves to stabilize the structure again and avoid complications. The article does not call surgery into question, but adds a functional perspective. - Why can a hernia come back after surgery?
A relapse can have various causes. These include tissue quality, healing process, stress after the operation, but also unfavorable pressure and tension conditions in the body. If the pressure continues to act on the same area, even a repaired structure can be strained again. - Are modern laparoscopic operations fundamentally better than traditional procedures?
Not necessarily. Modern procedures have many advantages, but are not subjectively more comfortable for every patient. Some people find traditional, open surgical methods better tolerated. The decisive factor is not only the technique, but also how the body reacts to it. - Why do people often feel insecure for a long time after a successful operation?
Because although an operation repairs structure, it does not automatically restore movement patterns, tension and confidence. The body „remembers“ the weak point and often works with caution for a long time. This is a natural protective mechanism. - What does the term body statics mean in this context?
Body statics describes how forces, pressure and tension are distributed in the body. If this distribution is unfavorable, overloading occurs at transition points such as the groin, pelvis or abdominal floor. Statics is not a specialized topic, but a fundamental principle of load and stability. - What role does the pelvis play in groin problems?
The pelvis is a central switching point between the upper body and legs. Changes in the pelvic position can influence where pressure is directed when straining, coughing or carrying. Unfavorable pelvic statics can put the groin under permanent tension. - What does coughing have to do with hernias or statics?
Coughing creates high pressure in the abdomen for a short time. Where this pressure is felt says a lot about the distribution of tension in the body. If the pressure is clearly felt in the groin, this may indicate a functional weakness or unfavorable statics. - Why can complaints shift over time?
Pressure in the body does not disappear, it is redirected. If statics or tension change, the location of the complaints can also change. This does not mean that a problem „moves“, but that the body compensates differently. - What do hemorrhoids and hernias have to do with each other?
Both issues are often associated with increased pressure in the lower abdominal and pelvic area. If this pressure is permanently distributed unfavorably, various symptoms can occur. The cause is often not the symptom itself, but the distribution of pressure. - Can a CMD splint actually have an effect on the rest of the body?
A CMD splint changes the bite position and therefore the position of the lower jaw. As the head is a central weight in the body system, the posture of the spine, pelvis and entire body can also change over time. This is not a quick effect, but a long-term process. - Does this mean that a CMD splint can „cure“ groin problems?
No. A CMD splint is not a treatment for hernias. However, it can have an indirect influence on statics and tension patterns. The article does not describe a cure through the splint, but a long-term change in the pressure conditions. - Why does breathing play a role in these topics?
Breathing influences the pressure in the abdominal cavity and the work of the diaphragm. Shallow, tense breathing can direct pressure downwards and strain sensitive areas. Functional breathing can help to distribute pressure more evenly. - When should you consult other specialists in addition to doctors?
If complaints keep recurring or do not disappear completely despite successful surgery, it may make sense to consult someone who takes a holistic view of the body. This could be an experienced osteopath or orthopaedist with a static focus. - Is this a criticism of conventional medicine?
No. The article is expressly intended as a supplement, not as a counter-proposal. Conventional medicine is strong in diagnosis and structural repair. However, functional correlations over long periods of time are naturally considered less frequently. - What is the most important insight from this personal story?
That symptoms are often clues, not isolated defects. A hernia can be the point at which a major imbalance becomes visible. If you are prepared to look further, you will often find new approaches beyond the mere treatment of symptoms. - What makes this article particularly valuable for those affected?
He combines medical reality with personal long-term experience, without promising a cure or apportioning blame. He shows that there can be a way forward even after setbacks - sometimes more slowly, sometimes unexpectedly, but often more sustainably than expected.